WELCOME TO HEAD & NECK ROBOTIC SURGERY IN THE H&N
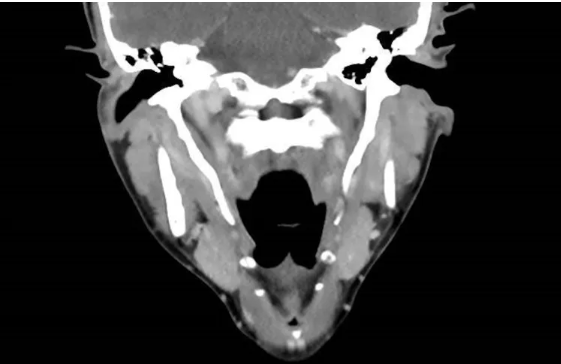
Eagle’s syndrome arises from an anomalous calcification of the stylohyoid ligament, leading to the anatomical elongation of the styloid process. While this condition is generally considered an anatomical variation in asymptomatic individuals, it may manifest with diverse symptoms attributable to the presence of a rigid structure in the upper neck. Common manifestations include swallowing disturbances, pain, and a sensation of a foreign body. Additionally, vascular symptoms may arise due to compression of the major vessels in the neck.
Surgical resection is the primary treatment for Eagle’s syndrome. However, this procedure is performed in proximity to critical structures such as the internal carotid artery, internal jugular vein, and lower cranial nerves in the retro-styloid space, which poses a risk of severe complications, including the potential for mortality.
Traditional surgical approaches, conducted through the neck, required the retraction of the vessels to access the styloid process safely. But yes, vital structures were controlled under direct visualization.
Transoral approaches have faced criticism for their limited visualization of the surgical field and reduced maneuverability, potentially jeopardizing neurovascular structures. Adding a potential risk of deep space neck infection (which has not been described, as far as I know…). For many years the transoral approach has been the approach of choice for may surgeons (including the one writing).
With the advent of Transoral Robotic Surgery (TORS) there is no longer room for criticism. It addresses these concerns by offering a minimally invasive approach with exceptional visual control and dexterity. TORS allows to access to the elongated styloid from anterior and medial, avoiding the exposure of the retro-styloid space. Actually, surgery is quite straightforward. See how it is done.
Some references on TORS management of lingual thyroid
Park YM, Kim WS, Byeon HK, Lee SY, Kim SH. A novel technique for the resection of the symptomatic lingual thyroid: transoral robotic surgery. Thyroid. 2013;23: 466-471. doi: 10.1089/thy.2012.0292.
Howard BE, Moore EJ, Hinni ML. Lingual thyroidectomy: the Mayo clinic experience with transoral laser microsurgery and transoral robotic surgery. Ann Otol Rhinol Laryngol. 2014;123:183-187. doi: 10.1177/0003489414522976.
Ersoy Callıoglu E, Bozdemir K, Ulusoy B, Oguzhan T, Korkmaz MH. Lingual Thyroid Excision with Transoral Robotic Surgery. Case Rep Otolaryngol. 2015;2015:548582. doi: 10.1155/2015/548582.
Vincent A, Jategaonkar A, Kadakia S, Ducic Y. TORS excision of lingual thyroid carcinoma: Technique and systematic review. Am J Otolaryngol. 2019 May-Jun;40(3):435-439. doi: 10.1016/j.amjoto.2019.02.013
Filarski CF, Levine B, Buttan A, Gonzalez NR, Ho AS. Enlarged hemorrhagic lingual thyroid managed with transoral robotic surgery. Endocrine. 2021 Jun;72(3):923-927. doi: 10.1007/s12020-020-02586-w.
D’Andréa G, Vairel B, Vandersteen C, Chabrillac E, Vergez S, Bonnecaze G. Is Transoral Robotic Surgery the Best Surgical Treatment for Lingual Thyroid? A Case-Report and Literature Review. Ann Otol Rhinol Laryngol. 2022 Jan;131(1):39-51. doi: 10.1177/00034894211007251
Curtis J, Walford S, Howe D. Transoral robotic resection of a lingual thyroid: a novel treatment for obstructive sleep apnoea. BMJ Case Rep. 2021 Sep 16;14(9):e241412. doi: 10.1136/bcr-2020-241412
Check open surgery alternative (free full text on PMC)
Kumar LK, Kurien NM, Jacob MM, Menon PV, Khalam SA. Lingual thyroid. Ann Maxillofac Surg. 2015 Jan-Jun;5(1):104-7. doi: 10.4103/2231-0746.161103.
… please, don´t if you can opt for minimal access surgery.
References
Park YM, De Virgilio A, Kim WS, Chung HP, Kim SH. Parapharyngeal space surgery via a transoral approach using a robotic surgical system: transoral robotic surgery. J Laparoendosc Adv Surg Tech A. 2013 Mar;23(3):231-6. doi: 10.1089/lap.2012.0197
Kamil RJ, Gonik NJ, Lee JS, Shifteh K, Smith RV. Transoral resection of stylopharyngeus calcification: a unique manifestation of a stylohyoid complex syndrome. Ann Otol Rhinol Laryngol. 2015 Feb;124(2):158-61. doi: 10.1177/0003489414546399
Kim DH, Lee YH, Cha D, Kim SH. Transoral robotic surgery in Eagle’s syndrome: our experience on four patients. Acta Otorhinolaryngol Ital. 2017 Dec;37(6):454-457. doi: 10.14639/0392-100X-1502
Kadakia S, Jategaonkar A, Roche A, Chai RL. Tonsillectomy sparing transoral robot assisted styloidectomy. Am J Otolaryngol. 2018 Mar-Apr;39(2):238-241. doi: 10.1016/j.amjoto.2018.01.007
Fitzpatrick TH 4th, Lovin BD, Magister MJ, Waltonen JD, Browne JD, Sullivan CA. Surgical management of Eagle syndrome: A 17-year experience with open and transoral robotic styloidectomy. Am J Otolaryngol. 2020 Mar-Apr;41(2):102324. doi: 10.1016/j.amjoto.2019.102324
Montevecchi F, Caranti A, Cammaroto G, Meccariello G, Vicini C. Transoral Robotic Surgery (TORS) for Bilateral Eagle Syndrome. ORL J Otorhinolaryngol Relat Spec. 2019;81(1):36-40. doi: 10.1159/000493736
Rizzo-Riera E, Rubi-Oña C, García-Wagner M, Costa AA, Miralles J, Enchev E, Rama-López J. Advanced Robotic Surgery of the Parapharyngeal Space: Transoral Robotic Styloidectomy in Eagle Syndrome. J Craniofac Surg. 2020 Nov/Dec;31(8):2339-2341. doi: 10.1097/SCS.0000000000006804
Campisi R, Caranti A, Meccariello G, Stringa LM, Bianchini C, Ciorba A, Pelucchi S, Vicini C. Transoral robotic styloidectomy for Eagle syndrome: A systematic review. Clin Otolaryngol. 2024 Jan 30. doi: 10.1111/coa.14145. Epub ahead of print. PMID: 38290994